Authors / metadata
DOI: 10.36205/trocar7.vid2601
Abstract
A rudimentary horn pregnancy is a rare and high-risk form of ectopic gestation that frequently evades early detection and carries a significant risk of uterine rupture. An exceptionally early diagnosis of a non-communicating rudimentary horn pregnancy at four weeks and four days, identified during evaluation for pregnancy of unknown location is presented. A 34-year-old woman was diagnosed with irregular β-hCG kinetics and an absent intrauterine gestational sac on initial ultrasonography. Targeted imaging demonstrated a tiny gestational sac within a left non- communicating rudimentary horn. Diagnostic hysteroscopy confirmed a unicornuate uterine cavity, and laparoscopy verified the ectopic implantation. Definitive management consisted of laparoscopic excision of the rudimentary horn with ipsilateral salpingectomy, performed with careful dissection along the horn–uterus junction, identification of ureteric peristalsis, and confirmation of contralateral tubal patency. The postoperative course was uneventful, and the patient subsequently achieved a term intrauterine pregnancy. This video highlights critical steps in early recognition and minimally invasive management of rudimentary horn pregnancy, underscoring the importance of targeted imaging, prompt diagnosis and standardized laparoscopic technique to prevent rupture and optimize reproductive outcomes.
Introduction
Rudimentary horn pregnancy is one of the rarest and most hazardous forms of ectopic gestation, with an estimated incidence of 1 in 76,000 – 150,000 pregnancies (1). It occurs almost exclusively in association with an unicornuate uterus, a Müllerian anomaly representing 2.4–13% of uterine malformations, up to 90% of all rudimentary horns are non-communicating, predisposing to occult implantation and early rupture (2,3). Conception within a non-communicating horn results from transperitoneal migration of sperm or a fertilized ovum (4). The hypoplastic myometrium limits distensibility, contributing to rupture rates of 50–90%, typically between 10–20 weeks of pregnancy, often before a diagnosis has been established (1,3). Diagnosis is challenging, as two-dimensional ultrasonography detects only 26% – 33% of cases and may mimic tubal or cornual ectopic pregnancy (2,5). Tsafrir’s criteria – pseudobicornuate configuration, a surrounding myometrial mantle and absent cervical continuity – aid early recognition but require expertise (5), while 3D ultrasonography and MRI further enhance diagnostic accuracy (6,7). An exceptionally early (four weeks four days) diagnosis of a non-communicating rudimentary horn pregnancy identified during evaluation for a pregnancy of unknown location is reported.
Case report
A 34-year-old G2P1 presented with 1 1/2 months of amenorrhea without pain or bleeding. Her history included an uncomplicated term vaginal delivery, laparoscopic detorsion of a twisted dermoid cyst (struma ovarii) ten years earlier, and a hysteroscopic metroplasty five years prior. Initial transvaginal ultrasonography did not reveal an intrauterine gestational sac, and she was classified as having a pregnancy of unknown location at four weeks and four days pregnancy. Serial β-hCG values rose from 53 to 2357 mIU/mL over ten days, but with irregular increments ranging from 11% to 76%, prompting concern for an ectopic pregnancy. Repeat transvaginal imaging demonstrated a unicornuate uterus with a separate left rudimentary horn containing a 1.8-mm gestational sac the left ovary showed a corpus luteum and both ovaries had polycystic morphology (Figure 1).
Diagnostic hysteroscopy confirmed a unicornuate right uterine cavity with a single right tubal ostium. Laparoscopy identified a non-communicating left rudimentary horn, which was excised together with the ipsilateral tube, chromopertubation confirmed right tubal patency. Postoperatively, β- hCG declined by 76% within 24 hours. Histopathological examination of the excised specimen confirmed the presence of chorionic villi and trophoblastic tissue within the rudimentary horn, consistent with an ectopic pregnancy (Figure 2).
The patient received routine postoperative care and follow-up. No contraception was advised, as the excision of a non-communicating rudimentary horn does not contraindicate future pregnancies nor adversely affect reproductive outcomes in the normally developed unicornuate uterus. She conceived spontaneously six months following surgery and subsequently had an uncomplicated term vaginal delivery.
Discussion
Surgical excision of a non-communicating rudimentary horn remains the definitive management in view of the substantial risk of rupture and associated maternal morbidity. Operative complexity is due to the distorted pelvic anatomy, the variable vascularity and the inconsistent fibromuscular attachment between the horn and the unicornuate uterus (6,8). The gravid horn is characteristically hypervascular, heightening the risk of intraoperative hemorrhage, and visualization may be further compromised in the presence of rupture or hemoperitoneum (9,10). At very early gestations, transvaginal ultrasound (TVUS) remains the first-line imaging modality for suspected ectopic pregnancy. In the present case, high-resolution TVUS combined with serial β-hCG measurements were sufficient to raise strong suspicion of a rudimentary horn pregnancy despite the early gestational age. Although MRI can aid in delineating Müllerian anomalies, it was deferred as it was unlikely to alter management and could delay definitive treatment. Direct endoscopic evaluation provided real-time anatomical confirmation, rendering additional cross-sectional imaging unnecessary (5). Conventionally, suspected rudimentary horn pregnancies are evaluated using a stepwise approach comprising ultrasonography, adjunctive MRI, and delayed laparoscopy. In contrast, the integrated same-setting hysteroscopy–laparoscopy workflow used in this case enabled immediate correlation between intrauterine and extrauterine anatomy, confirmed the absence of a communicating horn and allowed definitive management in one single procedure, thereby minimizing diagnostic delay and rupture risk (2,5). Once a rudimentary horn pregnancy is suspected, conservative or medical management is generally discouraged because rupture is unpredictable and frequently catastrophic. Medical management with methotrexate has demonstrated variable success and does not mitigate the inherent structural risk posed by a gravid rudimentary horn (1,11). Consequently, surgical excision was favoured even at four weeks and four days gestation to prevent progression to rupture and to achieve definitive treatment under controlled conditions. Although the patient was asymptomatic, rising β-hCG levels and clear anatomical suspicion supported early semi-urgent laparoscopy, allowing minimally invasive excision and avoidance of emergency surgery. Laparoscopic excision is the preferred modality in hemodynamically stable patients, supported by evidence demonstrating its safety, feasibility, and superior visualization (6,9,10). Conversely, laparotomy is indicated in unstable or ruptured presentations to facilitate prompt hemorrhage control. As rupture frequently results from delayed diagnosis, early identification is critical and enables minimally invasive intervention before significant bleeding ensues (12). Early diagnosis of a rudimentary horn pregnancy remains uncommon. Most reported cases are diagnosed after rupture or beyond eight to ten weeks gestation. Even in contemporary series using high-resolution ultrasonography, prerupture diagnosis is typically achieved at or beyond six to seven weeks. Diagnosis during the very early first trimester has been reported only in isolated cases (12-14). Diagnosis at four weeks four days as in the present case therefore represents an exceptionally early identification, permitting definitive laparoscopic management prior to rupture. Optimal surgical practice entails comprehensive preoperative imaging, meticulous intraoperative identification of the ureter and pelvic vasculature, and conservative use of energy devices near the unicornuate uterus to preserve tissue integrity. Postoperative counselling should address reproductive prognoses and emphasize the need for early targeted imaging in subsequent pregnancies. Overall, laparoscopic excision is the most appropriate approach for stable patients, with laparotomy reserved for emergency presentations, and early diagnosis remains the principal determinant of favourable outcomes.
Conclusion
Rudimentary horn pregnancy is an uncommon but potentially life-threatening form of ectopic gestation that often evades early diagnosis. In patients presenting with pregnancy of unknown location and atypical β-hCG rise, this condition must be considered. Early identification allows timely minimally invasive surgical intervention, preventing rupture and preserving reproductive potential. This case demonstrates the value of integrated hysteroscopic and laparoscopic evaluation and provides a stepwise operative approach through an accompanying instructional video.
Video
References
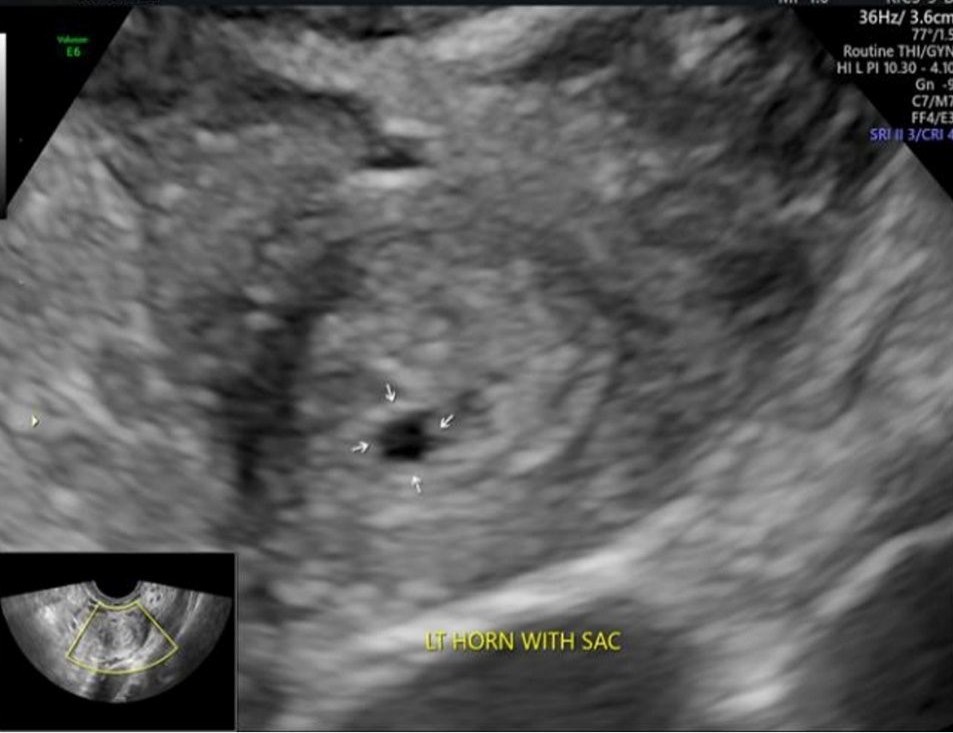
Figure 1. Transvaginal ultrasonography showing a left non-communicating rudimentary horn containing an early gestational sac (arrows)
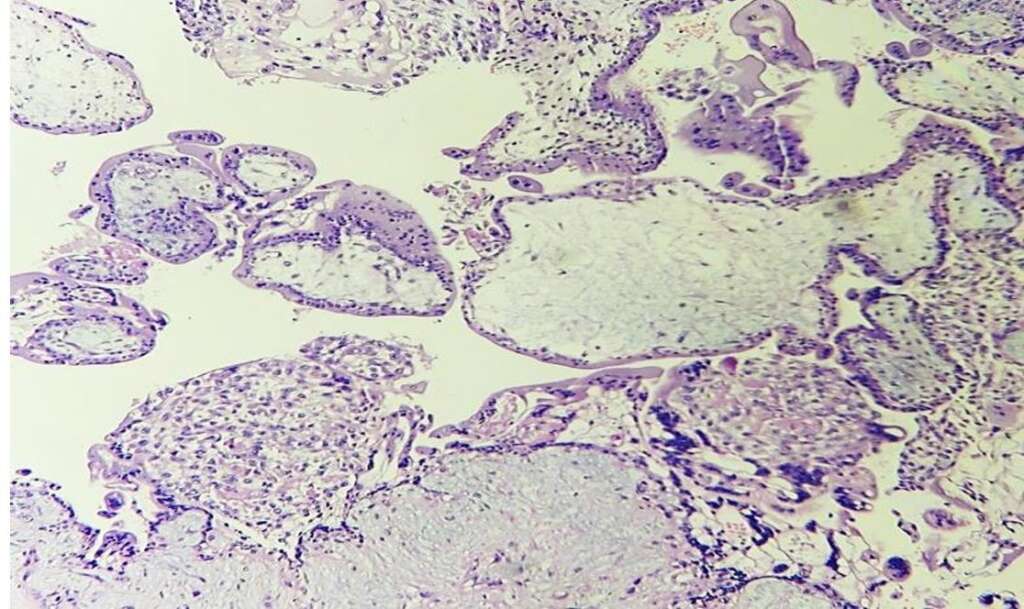
Figure 2. Histopathology of the excised specimen demonstrating chorionic villi with trophoblastic tissue, confirming ectopic pregnancy (H&E stain)