Authors / metadata
DOI: 10.36205/trocar7.2026003
Abstract
Uterine leiomyomas are the most frequent benign tumors of the female genital tract. However, their localization in the broad ligament is rare, and when they reach giant dimensions, these represent a diagnostic and surgical challenge. The case of a 51-year-old woman with abnormal uterine bleeding over a long period in time, refractory to medical treatment is presented. Pelvic ultrasound revealed a large uterine mass measuring 18.6 × 8.4 × 11.8 cm, hindering adequate visualization of the uterus and adnexa. A total laparoscopic hysterectomy was performed, during which a giant fibroid occupying the left broad ligament and a parasitic leiomyoma attached to the right pelvic wall were identified and successfully removed, with an estimated blood loss of 1,000 ml. Histopathology confirmed conventional uterine leiomyomatosis with degenerative changes and associated adenomyosis. The patient evolved favourably and was discharged 48 hours after surgery without complications. This case highlights the rarity of giant leiomyomas in the broad ligament, their potential to mimic adnexal or retroperitoneal tumors, and the feasibility of laparoscopic management as a safe and effective alternative in expert hands, even in highly complex scenarios.
Introduction
Uterine leiomyomas are the most common benign tumors of the female genital tract and develop from the smooth muscle of the myometrium. It is estimated that between 20% and 30% of women of reproductive age will develop this pathology, although the prevalence may vary depending on age, race and hormonal factors (1). Most leiomyomas are intrauterine. However, a small percentage are located outside the uterus and are considered extrauterine tumors. Among these, the ones that develop in the broad ligament are the most common, although their overall frequency is less than 1% of all cases of myomatosis (2). The broad ligament is a peritoneal fold that contains vital structures such as the ureters and uterine and ovarian vessels. Therefore, the growth of a leiomyoma in this location can alter normal pelvic anatomy and cause nonspecific symptoms. Clinically, these lesions can mimic adnexal tumors, ovarian cysts, or even retroperitoneal neoplasms (3). In addition, when leiomyomas reach large dimensions or present degenerative changes (such as necrosis or cystic degeneration), the clinical and imaging diagnosis becomes even more challenging (4). Diagnostic imaging, especially ultrasound and CT, can guide suspicion. However, it often fails to define the tumour’s origin with certainty. Magnetic resonance imaging is the most effective technique for characterizing soft tissue lesions and differentiating between leiomyomas and malignant tumors, although it is not always universally available (5). Given these limitations, definitive confirmation is established intraoperatively and with histopathological diagnosis. The rarity of giant leiomyomas of the broad ligament and their tendency to be confused with malignant tumors make case reports of great scientific value. The latter contribute to broadening our understanding of the clinical manifestations, diagnostic options, and therapeutic possibilities concerning these leiomyomas. This paper describes a case of giant leiomyoma of the broad ligament with parasitic myoma, successfully managed by total laparoscopic hysterectomy, in accordance with the most recent evidence.
Case report
A 51-year-old female patient with no significant medical history presented for consultation with long-standing abnormal uterine bleeding, refractory to conservative medical management and significantly impacting her quality of life. A pelvic ultrasound (Figure 1) revealed the presence of a solid uterine mass measuring 18.6 × 8.4 × 11.8 cm, which prevented adequate visualization of the rest of the uterus, endometrium, and adnexa.
Given these findings and the persistence of symptoms, a total laparoscopic hysterectomy was performed. During the procedure, classified as highly complex, a large uterine fibroid was identified that completely occupied the left broad ligament, as well as a parasitic myoma located on the right pelvic wall. A myomectomy of the parasitic tumor was performed, followed by a total hysterectomy. The surgical specimen was removed by morcellation (Figure 2-7), weighing a total of 1,349 grams (Figure 8). The estimated intraoperative blood loss was 1,000 ml, with no additional complications.
The histopathological results reported: conventional histological uterine myomatosis with degenerative changes and associated adenomyosis. The patient had a favourable postoperative course and was discharged 48 hours later without complications. This case highlights the rarity of giant broad ligament leiomyomas and the importance of laparoscopic hysterectomy as a feasible alternative, even in highly complex surgical settings.
Discussion
The presented case adds to the existing literature highlighting the diagnostic difficulty of broad ligament leiomyomas due to their low frequency and the fact that their clinical and imaging characteristics are often confused with those of adnexal tumors, particularly malignant ovarian masses (6,7). In our case, ultrasound did not allow clear visualization of the uterus nor the adnexa, which is consistent with previous reports where the large size of the mass obscures key pelvic structures. An important characteristic is that broad ligament leiomyomas can be classified as true (originating in the ligament’s own tissue) or false (subserosal uterine fibroids growing between the ligament layers) (8). This distinction, although difficult to establish before surgery, has implications for the surgical technique and the possibility of complications, mainly due to the proximity of the ureters and pelvic vessels. In the literature, most of these cases have been treated by laparotomy, which allows a wide approach and control of vascular structures, but at the cost of greater morbidity and prolonged recovery (9,10). However, in recent years, successful laparoscopic approaches have been described in selected cases, even in large tumors, thanks to the improvement in energy technology, the capacity for safe morcellation and the accumulated experience in minimally invasive surgery (11). The case presented confirms this possibility, achieving complete resection, controlled bleeding and a short hospital recovery, despite being a highly complex surgery. Another notable aspect is the presence of a parasitic myoma, a finding that, although rare, has already been described and represents an additional challenge in treatment. These tumors may be vascularized by neighbouring structures, which increases the risk of bleeding and makes dissection difficult. Furthermore, the histopathological results did confirm degenerative changes, a common finding in large masses, which explains their atypical radiological appearance and the similarity to malignant lesions (12). Overall, the literature review reinforces that giant leiomyomas of the broad ligament should be considered in the differential diagnosis of complex pelvic masses. Adequate surgical planning, accurate identification of critical anatomical structures, and experience in minimally invasive surgery are the pillars for successful and safe management of these patients.
Conclusion
Giant leiomyomas of the broad ligament represent a rare entity that is often confused with malignant adnexal tumors, especially when they present degenerative changes. The case presented demonstrates how, through appropriate surgical planning and the use of advanced laparoscopic techniques, these can be treated safely and effectively. The reviewed literature reinforces this statement. Although laparotomy remains the most reported option, laparoscopy is a feasible option in expert hands, offering advantages in recovery and lower morbidity. This case provides further evidence supporting the role of minimally invasive surgery in the management of complex broad ligament masses.
Remark of the editor
In view of international regulations concerning the spillage of tissue fragments at power morcellation and their possible impact on the long term follow up of the individual patient it is necessary to perform mechanical morcellation in a specifically designed bag. If this reveals impossible laparotomy is advised.
References
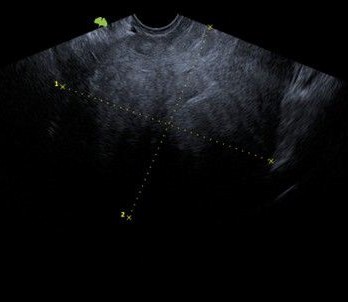
Figure 1: Pelvic Ultrasound reveals a large intraabdominal mass
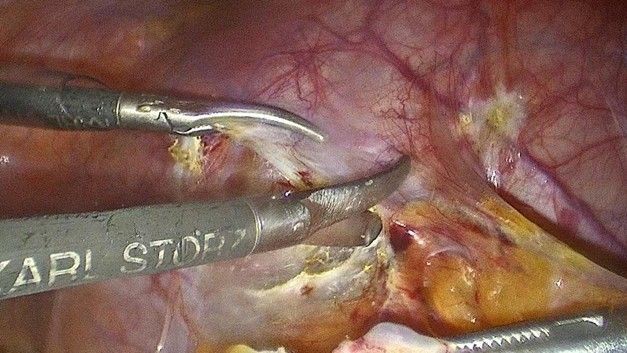
Figure 2: Close up of the surgical Instruments opening the peritoneum
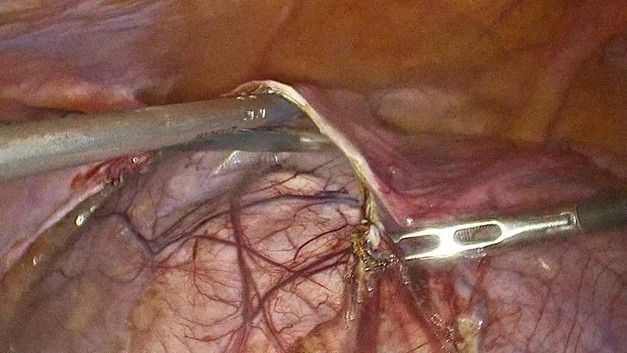
Figure 3: Decapsulating the parasitic leiomyoma

Figure 4: Close up of the decapsulation of the leiomyoma
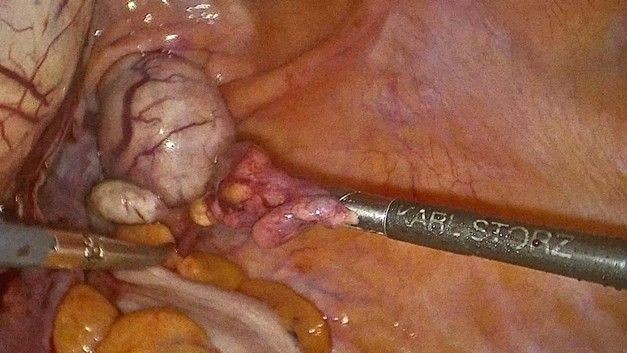
Figure 5: Starting the hysterectomy
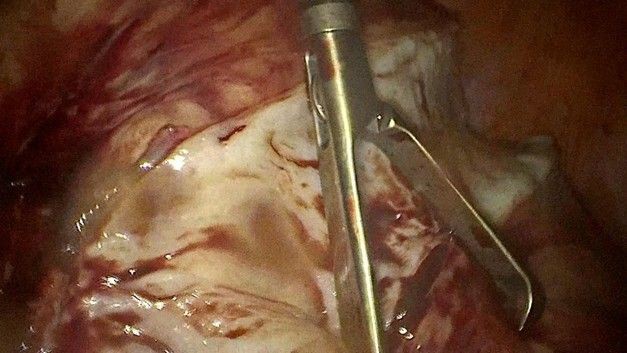
Figure 6: Starting the morcellation

Figure 7: Finishing the hysterectomy

Figure 8: The end result after morcellation