Authors / metadata
DOI: 10.36205/trocar7.2026008
Abstract
Transabdominal cervical cerclage is a therapeutic alternative for patients with cervical incompetence who have failed a previous transvaginal cerclage or who have anatomical limitations that prevent its performance. With the development of minimally invasive surgery, the laparoscopic approach has proven to be a safe and effective option, combining the benefits of obstetric management with the advantages of modern gynecological surgery. The case of a 36-year-old patient with a history of recurrent second-trimester miscarriages is presented. She underwent a laparoscopic transabdominal cerclage. The procedure was completed without complications, with minimal blood loss and rapid recovery, achieving a favorable obstetric outcome by letting the pregnancy continue to 38.5 weeks. The surgical technique is described step by step, highlighting key anatomical landmarks, relevant technical aspects, and recommendations to reduce the risk of complications. The available evidence supporting the effectiveness of this technique in prolonging pregnancy and improving perinatal outcomes in selected cases is also reviewed. It also highlights its advantages over the open approach, such as less postoperative pain, lower morbidity, and faster return to work. In conclusion, laparoscopic transabdominal cervical cerclage is emerging as a safe and effective option in appropriately selected patients. The integration of this case, the literature review, and the detailed technical description reinforce the role of minimally invasive surgery as a meeting point between obstetrics and surgical innovation.
Introduction
Cervical incompetence is an obstetric condition characterized by the inability of the cervix to remain closed during pregnancy. It affects approximately 1% of the population. It can cause second-trimester miscarriages and premature births, and its diagnosis is difficult as there is no definitive test (1,2). Premature birth, defined as birth before 37 weeks of gestation, is a leading cause of infant mortality and morbidity. There are a few effective strategies to prevent it, including cervical cerclage, introduced in the 1950’s, a common intervention used to prevent second-trimester pregnancy loss or premature birth (3). Transabdominal cerclage is a treatment option for cervical incompetence. It is recommended for patients with a previous transvaginal cerclage and spontaneous preterm birth before 28 weeks. It can be performed laparoscopically or open, depending on the gestational age and the experience of the surgeon (4). The laparoscopic approach offers the advantage of greater proximity to the internal cervical os and a lower risk of suture migration, lower morbidity, less blood loss, and faster recovery (5). In patients with refractory cervical incompetence, where traditional methods are ineffective, laparoscopic abdominal cerclage is an option. This procedure involves placing a suture around the cervix through a laparoscopic procedure (6). This technique has a live birth rate of 96.4% in patients who also underwent vaginal cerclage placement in a previous pregnancy. Average duration of the procedure is 26 +/- 4.7 minutes, with an average blood loss of 11.9 milliliters, and no reported infections, urinary tract injuries, or conversions to laparotomy (7). Transabdominal cervical cerclage by laparoscopy is as effective as that performed by laparotomy, but with lower surgical morbidity (2% of complications compared to 22% at laparotomy), so the choice of the method depends on surgical experience and discussion with the patient (8).
Case report
A 36-year-old female patient, G2 P1 A1, with no significant medical history. Her first pregnancy ended with a cesarean section at 27 weeks due to cervical incompetence, with a newborn weighing 850 g. She subsequently suffered an incomplete miscarriage at 19 weeks, also secondary to cervical incompetence, resolved by instrumental uterine curettage. Given the clear history of cervical incompetence, a laparoscopic transabdominal Benson-Durfee cerclage was performed. The procedure was performed without complications, the procedure lasted 60 minutes, a V Care type uterine mobilizer was used, with an estimated blood loss of 100 ml, and she was discharged the following day. Subsequently, the patient continued with follow-up and ultrasound confirmed the correct placement of the cerclage. (Figure 1).
The pregnancy progressed satisfactorily until 38.5 weeks, when a Caesarean section (CS) was scheduled. The newborn has a weight of 2930 g with an Apgar score of 8/9, with an estimated blood loss of 300 ml during the CS. The postoperative course was uneventful, and the patient was discharged 48 hours later in a good general condition. The surgical technique will be described step by step from the anatomical point of view.
- Preparation and access (Figure 2): The patient is placed in a modified dorsal lithotomy position, with a slight Trendelenburg position to facilitate pelvic exposure. Pneumoperitoneum is installed through the Palmer point access, and trocars are placed. The abdominal and pelvic cavities are assessed, identifying the uterus, adnexa, bladder, and rectum.
- Exposure of the lower uterine segment (Figure 3-5): the uterus is moved anteriorly or laterally to expose the utero-cervical junction (key anatomy: Anterior aspect of the lower uterine segment and cervix, vesicouterine fold, and peritoneal reflection of the bladder). The vesicouterine peritoneum is carefully incised and dissected, moving the bladder caudally to expose the anterior aspect of the cervix.
- Identification of lateral structures (Figure 6): Uterine arteries: These are located medially toward the uterus. It is essential to recognize them and maintain a meticulous dissection to avoid injury. Ureters: These are located laterally and posterior to the uterine vessels. It is important to always maintain indirect visualization and consider the avascular plane of the broad ligament. Working plane: This plane is defined between the uterine artery and the lateral insertion of the cervix, where the Mersilene tape will be placed.
- Mersilene Ribbon Pass (Figure 7-10): A 5 mm Mersilene tape (or similar) is used, mounted on a semicircular needle or introduced using a laparoscopic forceps, the needle is introduced from the anterior aspect of the isthmus-cervix to the posterior aspect, medial to the uterine artery and just superior and medial to the uterine insertion of the uterosacral ligament close to the level of the internal cervical os. Care is taken to avoid injuring uterine vessels or penetrating the cervical cavity. The procedure is repeated symmetrically on the contralateral side, passing the tape from posterior to anterior, always medial to the uterine artery.
- Securing the tape (Figure 11): The two ends of the tape are externalized on the anterior aspect of the cervix. They are tied firmly over the anterior aspect of the uterine isthmus, securing the cerclage without compromising cervical blood flow. It is recommended to tie two or three firm knots.
- Final review and closure (Figure 12-13): The absence of bleeding is verified along the dissection path and around uterine vessels, the vesicouterine peritoneum is repositioned over the dissected area, covering the tape knot, and trocars are removed under direct vision and the cavity is deflated.
- Key anatomical points: The safety plane lies medial to the uterine vessels, within the cervical stroma, but lateral to the cervico-isthmic junction. The ureter runs lateral and inferior to the broad ligament, so the tape must always be passed in the correct plane to avoid entrapment. The knot should be on the anterior surface of the uterine isthmus, protected by the vesicouterine fold.
Discussion
Cervical insufficiency remains a significant obstetric challenge due to its association with recurrent miscarriages and preterm births. In patients with failed transvaginal cerclage or unfavorable anatomical conditions, transabdominal cerclage represents an effective option, especially when performed laparoscopically. In a recent meta-analysis, Marchand et al. (2022) demonstrated that both open and laparoscopic transabdominal cerclage achieve neonatal survival rates approaching 95%, with significant improvements in gestational age and birth weight (9). While open transvaginal cerclage showed a greater reduction in preterm births, the laparoscopic approach offered advantages in postoperative recovery and hospital stay, reinforcing its role as the technique of choice in certain cases. Furthermore, another analysis by the same group showed that laparoscopy is associated with less intraoperative bleeding and a lower risk of major hemorrhage, reinforcing its safety compared to open transvaginal cerclage (10). Correct cerclage placement is a critical success factor. Demirel et al. (2023) reported a case in which the Mersilene tape inadvertently passed through the cervical canal, highlighting the importance of incorporating verification techniques such as hysteroscopy at the end of the procedure (11). In our case, correct placement was confirmed by ultrasound, with a satisfactory outcome until the pregnancy reached term. Regarding transvaginal techniques, McAuliffe et al. (2023) found that the Shirodkar cerclage is associated with a lower risk of preterm birth than the McDonald cerclage, particularly births before 35, 34, and 32 weeks, as well as higher birth weight (12). While the quality of the studies limits the strength of these conclusions, the findings reinforce the principle that suture height and firmness are determining factors for success, a concept that can be extrapolated to the Benson-Durfee transabdominal cerclage. Latin American evidence also supports the efficacy of this method. In a case series in Mexico, five cases of laparoscopic abdominal cerclage were reported, with a neonatal survival rate of 80% and a mean time to delivery of 37.2 weeks. Furthermore, the advantages of minimally invasive surgery over laparotomy were confirmed, such as less bleeding, less postoperative pain, and earlier return to work (13). These results are consistent with the case presented, where the patient progressed without surgical complications and achieved a full-term pregnancy with a good neonatal outcome. Regarding alternative approaches, vaginal progesterone and serial ultrasound measurements of cervical length remain cornerstones in the prevention of preterm birth in patients at risk of cervical insufficiency, especially those without prior surgical history or in whom invasive procedures are to be avoided. Likewise, the cervical pessary has emerged as a non-surgical intervention that may offer benefits in selected cases, although the evidence remains heterogeneous and its role is still debated. Similarly, several international guidelines suggest individualizing the therapeutic choice, considering factors such: as residual cervical length, patient preference and the availability of surgical expertise, emphasizing that transabdominal cerclage should be reserved for situations in which conservative or transvaginal alternatives are not feasible or have failed. Finally, the potentially catastrophic risks of transabdominal cerclage should not be underestimated. Dandapani et al. (2019) described a case of uterine rupture at term in a patient diagnosed by computed tomography who went into spontaneous labor, with serious maternal and fetal consequences (14). This report underscores the need for rigorous obstetric planning, with elective intervention before the onset of labor. In the case presented, a planned cesarean section at 38.5 weeks prevented this type of complication (1).
Conclusion
Laparoscopic Benson-Durfee transabdominal cerclage is confirmed as a safe and effective alternative in patients with cervical incompetence and a history of failed vaginal access. The evidence reviewed supports its ability to prolong gestation, improve neonatal survival, and reduce complications, with clear advantages over laparotomy thanks to the benefits of minimally invasive surgery. Our clinical case illustrates how proper patient selection, meticulous execution of the technique, and strict obstetric planning achieve favorable maternal and perinatal outcomes. In this sense, laparoscopic cerclage is positioned as a key tool at the intersection of obstetrics and minimally invasive surgery, always within a multidisciplinary approach and under specialized follow-up.
References
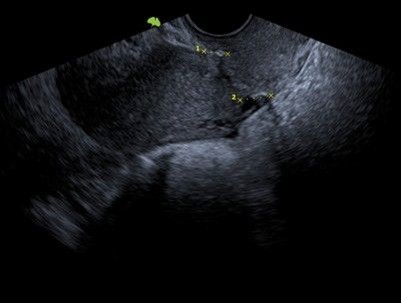
Figure 1: Green arrow: correct placement of the cerclage

Figure 2: preparation and access at Palmer’s point

Figure 3: exposure of the lower uterine segment
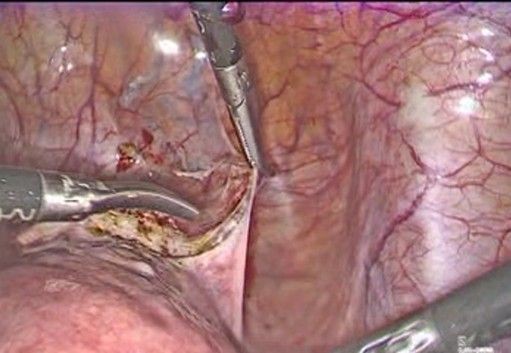
Figure 4: Careful incision of the bladder peritoneum
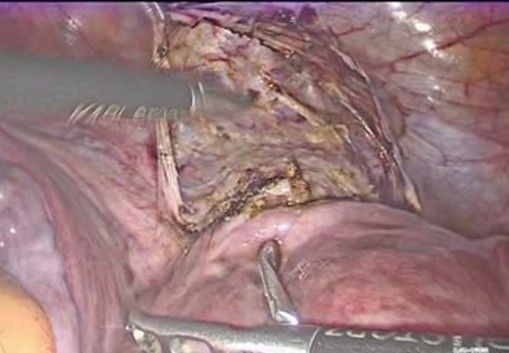
Figure 5: the bladder I moved caudally
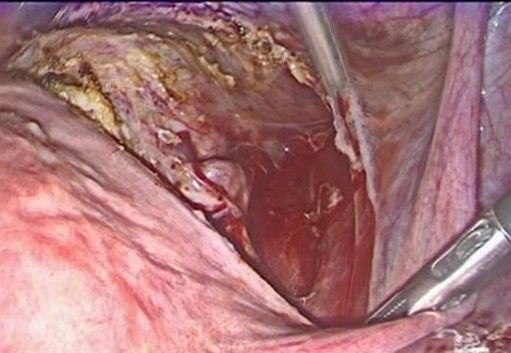
Figure 6: exposure of the uterine arteries
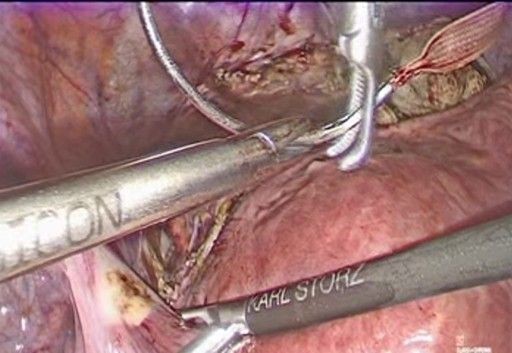
Figure 7: introduction of the 5 mm Mersilene tape
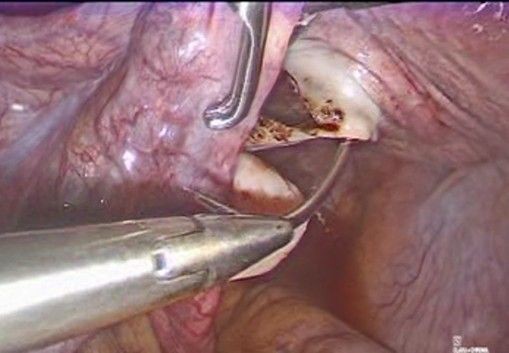
Figure 8: introduction of the needle in the anterior aspect of the cervix
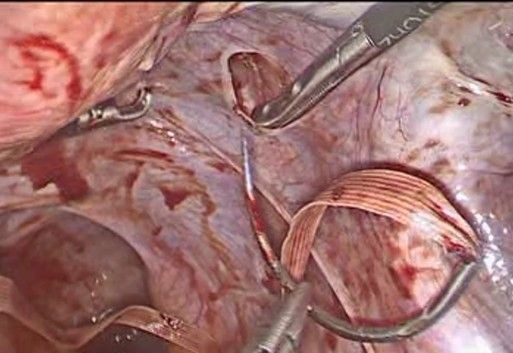
Figure 9: the needle passes from the anterior aspect of the isthmus-cervix to the posterior aspect, medial to the uterine artery and just superior and medial to the uterine insertion of the uterosacral ligament close to the level of the internal cervical os
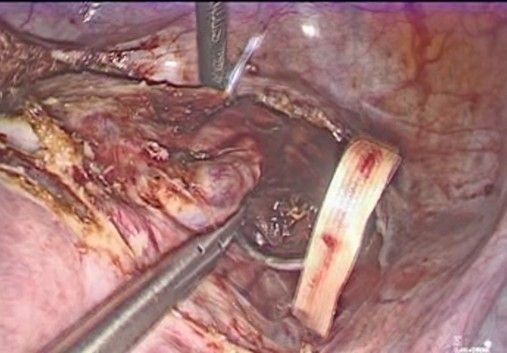
Figure 10: The needle is regrasped and brought back to anterior on the right side
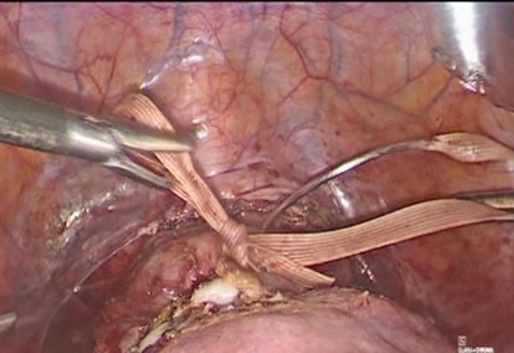
Figure 11: the knot is made to secure the tape
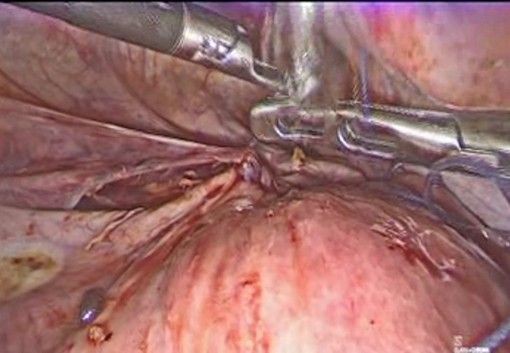
Figure 12: Repositioning of the vesicouterine peritoneum
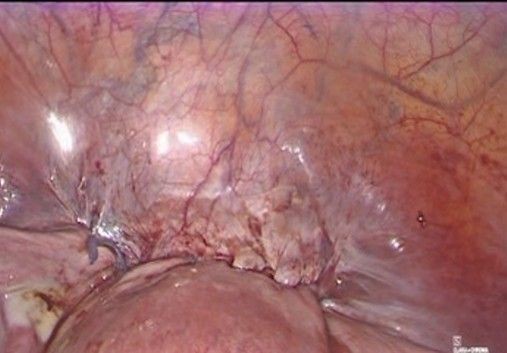
Figure 13: final aspect before removal of the trocars