Authors / metadata
DOI: 10.36205/trocar7.2026009
Abstract
Background: Deep infiltrating endometriosis (DE) involving the bowel presents a significant surgical challenge due to difficulty in accurately assessing the lesion’s depth and determining the appropriate extent of the bowel resection.
Material and Methods: The use of intraoperative endorectal ultrasound (Endo-USG) integrated with the robotic TilePro interface is described as a real-time guidance tool during robotic surgery for bowel endometriosis.
Clinical Application: Two patients with bowel DE underwent robotic surgery using the intraoperative Endo-USG guided surgical decision-making tool. In the first case, ultrasound confirmed muscularis involvement, prompting rectal disc excision. In the second case, Endo-USG demonstrated superficial disease despite preoperative MRI suggesting deeper infiltration, allowing conservative rectal shaving and avoidance of unnecessary bowel resection.
Conclusion: Robotic-integrated intraoperative Endo-USG may enable more appropriated real-time lesion characterization, and by giving more information supports tailored surgical strategies, and enhances precision in bowel endometriosis surgery. This technique may help to prevent overtreatment while ensuring complete disease excision.
Introduction
Deep infiltrating endometriosis (DE) involving the bowel affects approximately 8–12% of women with endometriosis and most commonly involves the rectosigmoid colon (1). Surgical management aims to achieve complete disease excision while preserving bowel function.
However, intraoperative assessment of bowel wall infiltration remains challenging, as visual inspection and palpation may underestimate lesion depth especially with less experienced surgeons (2). The choice between rectal shaving, disc excision, or segmental bowel resection is often based on preoperative imaging and intraoperative judgment. Inaccurate assessment may lead to incomplete excision or unnecessary radical bowel surgery, both of which can adversely affect patient outcomes (3). Intraoperative endorectal ultrasound (Endo-USG) provides real-time, high-resolution visualization of bowel wall layers, complementing visual assessment and improves accuracy of indepth evaluation (4). Integration of Endo-USG with robotic platforms using TilePro technology allows ultrasound images to be displayed simultaneously with the operative field on the surgeon’s console, enhancing precision and surgical confidence.This article describes a novel operative technique utilizing robotic-integrated intraoperative Endo-USG to guide real-time surgical decision-making in bowel endometriosis, illustrated through two clinical cases.
Materials and Methods
This report describes the application of a novel operative technique in two consecutive patients undergoing robotic surgery for bowel endometriosis at a tertiary referral center.
All procedures were performed using a robotic surgical platform equipped with TilePro visualization capability. Following standard robotic port placement and adhesiolysis, intraoperative endorectal ultrasound was performed using a transrectal ultrasound probe. Saline hydrodissection was used when necessary to enhance delineation of tissue planes.
Ultrasound images were displayed in real time on the robotic console using the TilePro interface, allowing simultaneous visualization of the operative field and ultrasound findings. Based on real-time assessment of lesion depth and bowel wall involvement, the surgical approach was tailored intraoperatively.
Results
Case 1: A 39-year-old G1P0A1L0 woman presented with severe dysmenorrhea, vaginismus, dysuria, dyschezia, and constipation refractory to medical therapy. Preoperative MRI demonstrated uterine adenomyosis with a superficial rectal plaque. During robotic surgery, dense adhesions in the rectovaginal space raised suspicion of deeper rectal involvement. Intraoperative Endo-USG revealed a hypoechoic lesion extending up to the muscularis layer of the rectum. Based on these findings, a robotic rectal disc excision was performed in collaboration with a colorectal surgeon. TilePro integration allowed confirmation of complete excision and rectal wall integrity. Histopathology confirmed muscularis-involving endometriosis. At one-year follow-up, the patient reported complete resolution of bowel symptoms.
Case 2: A 33-year-old unmarried woman presented with severe dysmenorrhea, right iliac fossa pain, and constipation. Preoperative MRI suggested deep infiltrating endometriosis with probable rectal muscularis involvement (Figure 1). Following saline hydrodissection, intraoperative Endo-USG demonstrated superficial mucosal involvement without muscularis infiltration (Figure 2). Based on these real-time findings, conservative rectal shaving was performed instead of the initially planned disc excision (Figure 3,4). Histopathology confirmed superficial endometriosis. At six-month follow-up, the patient reported marked improvement in dyschezia and constipation. Summary of the two cases in table 1 and comparison with the study data with data in literature in table 2.
Discussion
Surgical management of bowel endometriosis must be individualized according to the depth of bowel wall infiltration (3). Rectal shaving is appropriate for superficial disease, whereas disc excision or segmental resection is reserved for deeper infiltration. Accurate intraoperative assessment is therefore critical. In our experience, intraoperative Endo-USG provided real-time anatomical information that directly influenced intraoperative decision-making. In Case 1, ultrasound confirmed muscularis involvement, justifying disc excision. In Case 2, ultrasound findings contradicted preoperative MRI, allowing avoidance of unnecessary bowel resection. Previous studies have demonstrated the utility of intraoperative ultrasound in bowel endometriosis surgery (4). However, most reports describe laparoscopic ultrasound without robotic integration or post-excision assessment. The integration of Endo-USG with robotic TilePro technology could represent a significant advancement, as it enables continuous dual visualization of surgical anatomy and ultrasound findings without interrupting the surgical workflow (5). This approach may enhance surgical precision, reduces intraoperative uncertainty, and supports tailored, organ-preserving surgery. Although limited by the small sample size and short follow- up, this report demonstrates feasibility and possible clinical benefit.
Conclusion
Robotic-integrated intraoperative endorectal ultrasound may be a valuable adjunct in the surgical management of bowel endometriosis. By enabling real-time assessment of the lesion’s depth and bowel wall involvement, this technique may facilitate ta ailored surgical decision-making, prevent unnecessary radical resections, and enhance surgical precision. Wider adoption and structured evaluation of this technique has the potential to contribute to precision-guided minimally invasive endometriosis surgery.
References

Figure 1: Both sides rectal endometriotic nodule on MRI
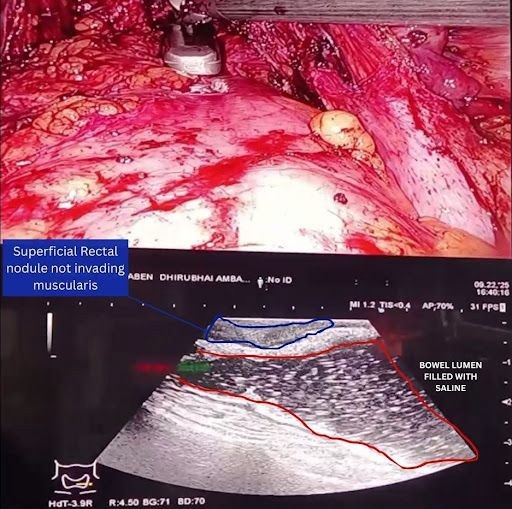
Figure 2: Intraoperative, robotic integrated ultrasound image with simultaneous view during surgery showing a superficial rectal nodule, not invading muscularis

Figure 3: Rectal shaving being performed
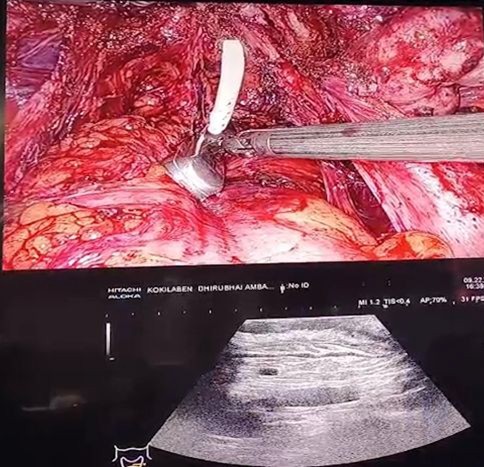
Figure 4: Completeness of the resection confirmed by US
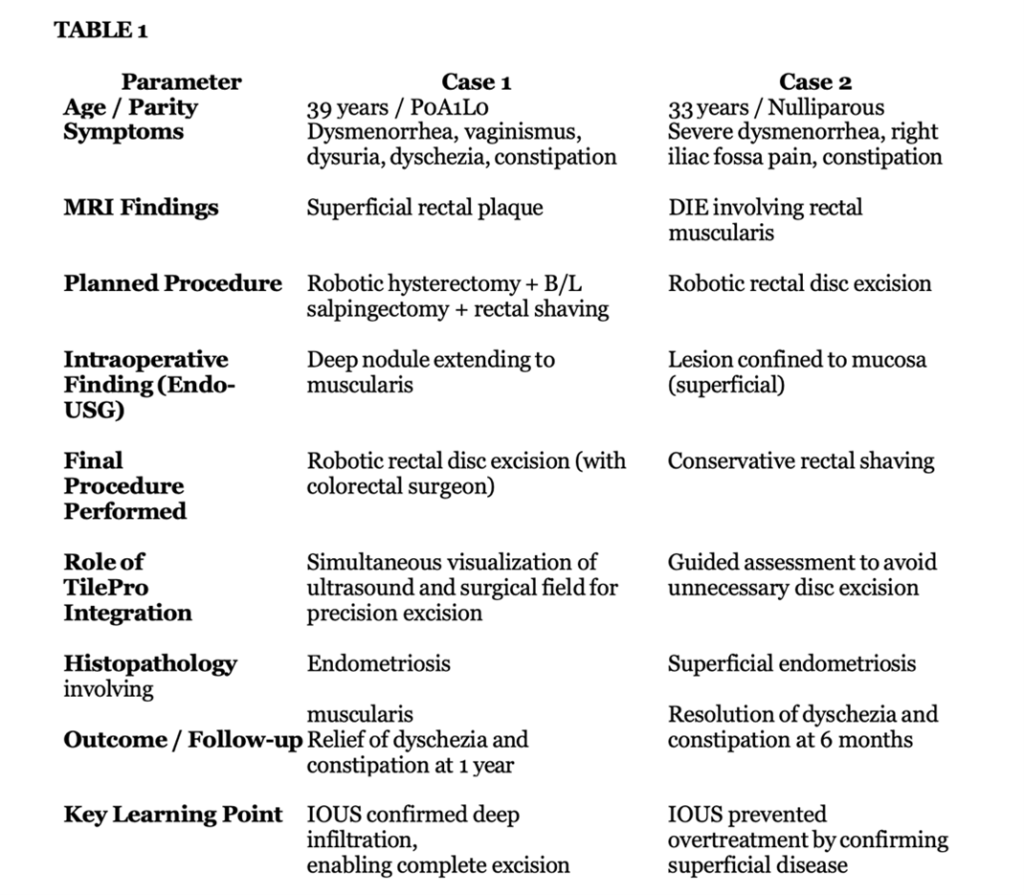
Different parameters of the two cases icluding pathology and followup
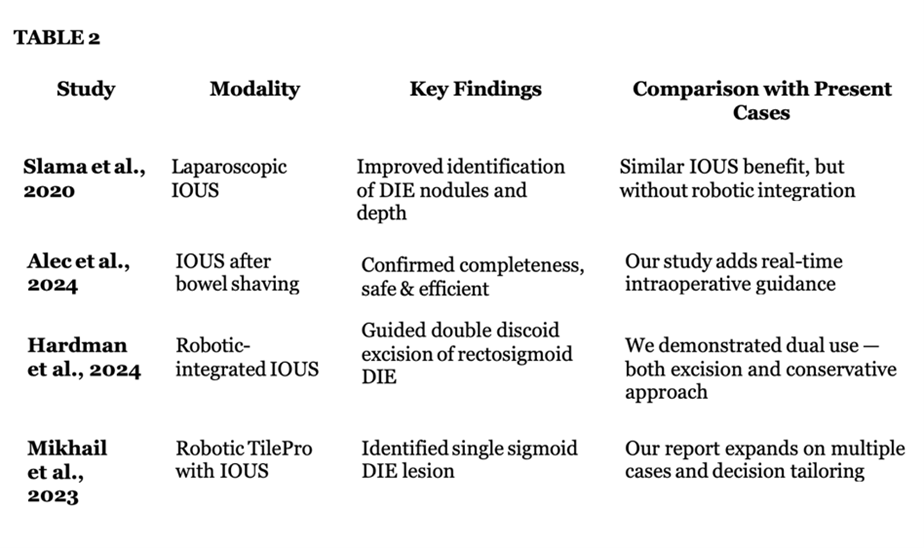
Comparison between different studies, different modalities of Intraoperative Ultrasound, Keyfindings in the literature and the comparison with the study at hand