Authors / metadata
DOI: 10.36205/trocar7.2026005
Abstract
Introduction: Uterine artery ligation prior to myomectomy is a crucial surgical step that significantly minimizes intraoperative blood loss and enhances operative safety. In laparoscopic myomectomy this can be achieved by uterine artery ligation. Conventionally this is achieved through retroperitoneal dissection and ligation of the artery at its origin from the internal iliac artery. However, in certain situations like a large impacted uterine myoma, limited uterine mobility and lack of experience in retroperitoneal dissection, this approach may not be feasible. The objective of this report is to describe an alternate and simplified method of uterine artery ligation at the level of the internal os (isthmus), which provides effective haemostasis without the need for retroperitoneal dissection. This technique thus offers a practical, safe, and efficient alternative in challenging cases, expanding the applicability of uterine artery ligation in minimally invasive myomectomy.
Study Objective: To describe and evaluate an alternative technique of uterine artery ligation at the isthmus in laparoscopic myomectomy, particularly for cases where retroperitoneal dissection and ligation at the artery’s origin is not feasible due to large uterine fibroid or lack of expertise.
Introduction
Uterine fibroids or leiomyomas are benign smooth muscle tumours of the uterus and represent the most common pelvic neoplasm in women of reproductive age, with a varying incidence of 20-40% in women over 30 years of age (1). Clinically fibroids may remain asymptomatic or present with symptoms like menorrhagia, dysmenorrhea, pelvic pain, pressure symptoms on bladder or bowel, infertility or adverse pregnancy outcomes (2). Effective haemostatic strategies in laparoscopic myomectomy are essential to ensure surgical efficacy and patient safety. Uterine artery ligation has proven to be a valuable technique to achieve significant and sustained reduction in uterine perfusion before myoma enucleation (3). The rationale for performing uterine artery ligation during laparoscopic myomectomy is grounded in its ability to reduce uterine blood flow without compromising uterine viability or future fertility. Conventionally ligation of the artery is done at its origin from the internal iliac artery (4). However, in our case where a large uterine fibroid obscured access to the retroperitoneal space we ligated the uterine arteries at the level of the isthmus, which offered a practical and effective means of achieving haemostasis.
Case report
A 32-year-old nulligravida presented with complaints of menorrhagia and pelvic pain persisting for the past three months. Her symptoms were not relieved by medication. On general examination, she appeared pale with stable vital signs. Abdominal examination revealed a firm, globular mass arising from the pelvis, corresponding to a uterine size of approximately 18 weeks’ gestation. Pelvic ultrasonography demonstrated a uterus measuring 8x7x6 cm, containing a fundal intramural fibroid measuring 12 cm in diameter. Preoperative evaluation revealed anaemia secondary to chronic blood loss. The patient was optimised with iron supplementation and scheduled for laparoscopic myomectomy. Under general anesthesia a ten mm supra umbilical port and four five mm accessory ports were inserted, a uterine manipulator was inserted vaginally. Upon laparoscopic entry, the pelvic space was markedly reduced due to the large impacted fundal fibroid, which completely filled the pelvis and caused negligible uterine mobility (Fig.1).
The retroperitoneal space was inaccessible precluding safe identification and dissection of the uterine artery at its origin due to an inaccessible retroperitoneal space because of size and weight of the myoma (Fig.2).
Given the anticipated risk of excessive intraoperative bleeding, bilateral uterine artery ligation at the level of the isthmus was planned and executed. The uterine mass was displaced cephalad to expose the uterine isthmus where adequate operative space was preserved. The uterine artery was identified by its prominent pulsations. Using the round ligament, uterovesical peritoneal fold and uterine artery as landmarks area of dissection was chosen (Fig.3).
The uterovesical peritoneal fold was incised and the bladder was carefully dissected and reflected inferiorly. At the level of the isthmus the ureter lies in close proximity to the uterine artery with the ureter lying 1.5 cm lateral to the uterine cervix (5). In order to increase this distance and safeguard the ureter during uterine artery ligation, it is important to apply traction either by pushing the uterine body away with a vaginal manipulator or by pulling it with a myoma screw. Furthermore, inferior mobilization of the bladder from the cervical surface results in lateral displacement of the ureters (Fig-4).
Adequate exposure at the isthmus is achieved by performing dissection both anteriorly and posteriorly. Anteriorly, the uterovesical peritoneal fold is incised and the bladder is mobilized inferiorly, while posteriorly the peritoneum over the uterosacral area is opened. This dual-plane dissection allows the ureter to fall laterally and inferiorly, thereby increasing the safety margin during ligation left and right uterine arteries seen pulsating at the level of internal os of cervix were identified and exposed. Blunt dissection was done between the uterine artery and vein to allow passage of suture under the artery without puncturing the vein (Fig 5).
A delayed absorbable suture polyglactin 910 (Vicryl no.1, code 2347, Johnson & Johnson, USA) was carefully passed under the artery remaining superficial to the myometrium and avoiding the uterine vein (fig 6). A regular knot was taken on the left (Fig 7) and a reversible uterine artery ligature (shoelace knot) on the right (6) (Fig 8).
The shoelace reversible knot has been shown to remain securely in place when applied around a well-dissected, isolated uterine pedicle at the origin of the uterine artery. However, in our experience so far when ligation is performed at the isthmus, as in our case, the vascular bundle is broader and less discrete, making the shoelace knot more prone to slippage. To ensure reliable haemostatic control in this location, we therefore opted for a permanent ligation on the left side.
At the same time, because this was a fertility-enhancing procedure, the aim was to restore uterine perfusion as much as possible postoperatively. For this reason, a shoelace reversible knot was applied on the right uterine artery, which was opened after myomectomy allowing at least unilateral re-establishment of blood flow after surgery. This approach balanced the need for secure intraoperative haemostasis with the patient’s reproductive goals. After successful ligation, the proximal portion of the uterine artery exhibited increased pulsatility, indicating a compensatory attempt to re-establish distal perfusion. Subsequently diluted vasopressin was injected into the myometrium surrounding the fibroid to further minimize capillary oozing and facilitate enucleation under a nearly bloodless field. A linear serosal incision was then taken over the most prominent part of the fibroid, fibroid capsule identified and dissected sharply. The fibroid was enucleated by traction and counter traction. The fibroid bed was inspected for any residual bleeding, which was minimal due to prior uterine artery ligation. The myometrial defect was closed in two layers with polyglactin sutures and haemostasis was confirmed. The excised fibroid was retrieved by contained in bag morcellation. The total intraoperative blood loss was 50 cc and no transfusion was required. The patient had an uneventful postoperative recovery, tolerated oral intake the same evening and was discharged on the second postoperative day. At three months follow up she reported normal menstrual cycles and resolution of pelvic pain, with no evidence of recurrence or postoperative complications.
Discussion
Intraoperative bleeding remains one of the most significant challenges during laparoscopic myomectomy. Among various haemostatic measures, uterine artery ligation has proven to be an effective and reliable technique to achieve sustained reduction in uterine blood flow. By devascularizing the uterus before myoma enucleation, it not only minimizes intraoperative bleeding but also improves surgical field clarity, reduces operative time and decreases the need for transfusion or repeated vasopressin injections. Bilateral uterine artery ligation offers additional advantages over unilateral occlusion, as it provides symmetrical and more complete reduction of uterine perfusion (7). Traditionally, the uterine artery is ligated at its origin from the internal iliac artery via three possible routes, anterior, lateral or posterior approach (8). The anterior approach is through the peritoneum over the obliterated umbilical ligament which is incised and the uterine artery is identified where it crosses over the ureter. The lateral approach describes the access to the uterine origin by incising the peritoneum between the round ligament, the infundibulopelvic ligament and the external iliac vessels. The posterior approach explains the dissection from the ovarian fossa using the ureter and the obliterated umbilical ligament as landmarks. Each of these methods demands meticulous dissection, experience and skill.
While vasopressin injection is commonly used for transient haemostasis, it has several limitations. Its effect is short lived and dependent on diffusion within the myometrium. Overdosage or inadvertent intravascular injection may cause systemic adverse effects such as hypertension, bradycardia, arrhythmia or even cardiac arrest. These systemic adverse effects can be avoided by using the visual vasopressor injection needle which has a transparent window close to the tip of the needle, allowing the surgeon to immediately see blood in this window during surgery, in case of accidental vessel puncture and immediately withdrawing and repositioning it (9). Moreover, in large or degenerated fibroids, vasopressin distribution maybe uneven, resulting in incomplete haemostasis. The uterine artery itself exhibits considerable anatomical variation, both in its origin and branching pattern. It may arise from the internal iliac, umbilical, inferior gluteal, or even the vaginal artery and its course relative to the ureter can vary (10). These variations coupled with limited pelvic space or a large impacted fibroid may render retroperitoneal identification technically challenging or unsafe. In such scenarios, uterine artery ligation at the level of the isthmus serves as a valuable and simplified alternative. This approach avoids the need for extensive retroperitoneal dissection while providing the same haemostatic benefit. This technique is particularly advantageous when large fibroids obscure the pelvic space or restrict uterine mobility. The isthmic approach ensures effective control of uterine perfusion, reduces intraoperative blood loss, and maintains procedural safety even in complex anatomical situations. Concerns have been raised regarding the potential impact of bilateral uterine artery ligation on fertility and uterine function. However multiple studies have demonstrated that collateral revascularization of the uterus occurs within weeks after ligation, preserving endometrial receptivity and ovarian perfusion (11). In our technique also due to isolated uterine artery ligation ovarian reserve is preserved. Clinical evidence indicates that fertility outcomes remain unaffected, making bilateral uterine artery ligation a safe procedure in women desiring future conception. The argument that a reversible bilateral artery ligation may be better still continues and needs further research and evidence.
Conclusion
Uterine artery ligation is a pivotal step in minimising intraoperative blood loss during laparoscopic myomectomy. While ligation at the artery’s origin remains the conventional technique, it may not always be feasible in cases with large or impacted fibroids that restrict retroperitoneal access. In such situations, bilateral uterine artery ligation at the level of isthmus offers a safe, simple and effective alternative that ensures excellent haemostasis without compromising uterine integrity or fertility. This approach reduces operative difficulty, avoids the risks associated with deep pelvic dissection and. Vasopressin use and broadens the applicability of laparoscopic myomectomy even in complex surgical scenarios.
References

Figure 1: Impacted pelvic mass

Figure 2: Inaccessible retroperitoneal Space due to size and weight myoma

Figure 3: Identifying the area of dissection using the round ligament and the uterovesical peritoneal fold as landmarks
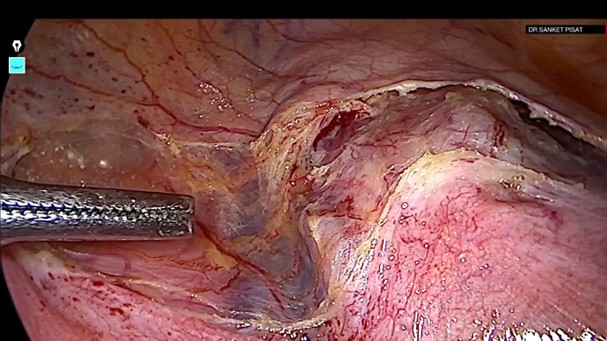
Figure 4: Uterovesical peritoneal fold incised and bladder dissected inferiorly, exposing the uterine artery and vein
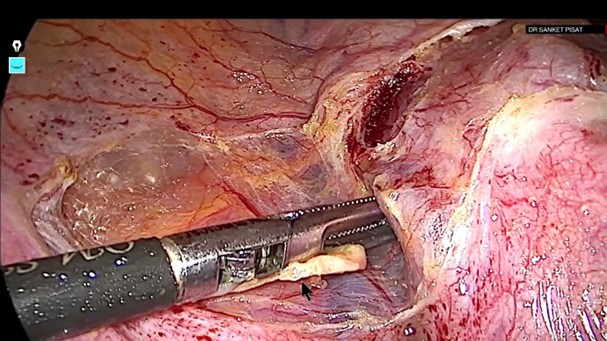
Figure 5: Blunt dissection done between the uterine artery and vein
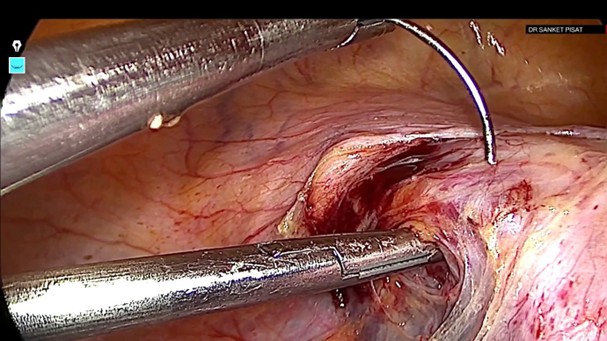
Figure 6: The needle is carefully passed under the left uterine artery while avoiding injury to the uterine vein
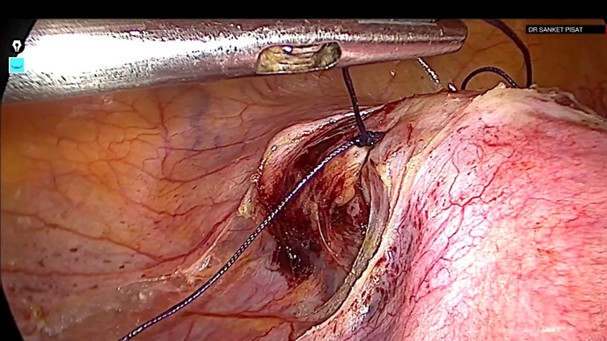
Figure 7: Left uterine artery ligated With a regular knot
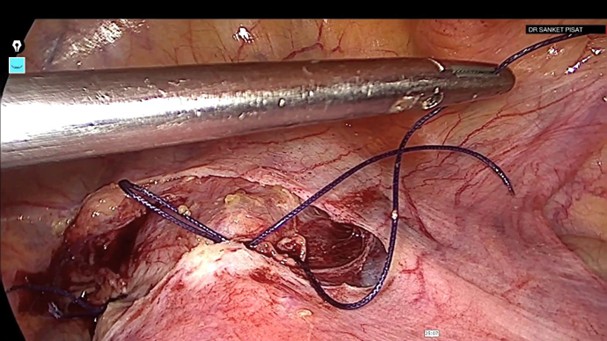
Figure 8: – Right uterine artery ligated with a reversible shoelace knot