Authors / metadata
DOI: 10.36205/trocar7.2026000
Abstract
Purpose: Chronic pelvic pain (CPP) is a common and debilitating gynaecological condition, for which diagnostic laparoscopy is the gold standard for diagnosis. In this study, the aetiology and perioperative complications among women undergoing diagnostic laparoscopy for CPP have been investigated.
Materials and Methods: A cross-sectional study was conducted at two tertiary hospitals in Harare, Zimbabwe, and included 108 women. In the retrospective arm (49 women), data were collected from hospital records, while in the prospective arm (59 women), data were collected prospectively. The findings were recorded and analysed using Stata version 12.0.
Results: Diagnostic laparoscopy confirmed pathological conditions in 81.6% of the women. The most frequent findings were ovarian pathologies (18.5%), endometriosis (15.7%) and adhesions (15.7%). Depression and anxiety were the psychological symptoms most commonly associated with CPP. The perioperative complication rate was low (0.06%). Conclusion. Most cases of CPP at the two institutions have a physical cause. Laparoscopy is a safe method for evaluating CPP.
Introduction
Chronic pelvic pain (CPP) affects approximately 15% to 24% of women worldwide (1,2). A study in Zimbabwe revealed that 35% of women had various reproductive pathologies on diagnostic laparoscopy (3). CPP is defined as persistent pelvic pain lasting at least 6 months, severe enough to limit function, and unrelated to menstruation or pregnancy. CPP management costs in the USA are estimated at $100 billion (4). The pathophysiology of CPP is unclear, but it is more prevalent in women with histories of substance abuse, miscarriages, heavy menstrual periods, abdominal surgery, abuse, and depression (5). Several concomitant psychological and physical disorders have been associated with CPP, with the most prevalent being depression (25%–50%), anxiety (10%–20%), multiple psychological disorders (20%–30%), and somatic disorders (10%–20%) (6). CPP conditions often overlap with non-pelvic pain disorders and non-pain conditions, contributing to pain severity. Musculoskeletal pain and dysfunction are observed in 50%–90% of patients with CPP (7). CPP affects women’s physical, psychological, and sexual health, as well as that of their partners (8). Management of chronic pain, and thus of CPP, requires a multidisciplinary approach (9). To date, research on CPP in Africa is limited. At the time of this current study (2014), diagnostic laparoscopy was widely regarded as the reference standard, particularly in low-resource settings with limited access to advanced imaging. Current practice recommends expert transvaginal ultrasound as a first-line for suspected endometriosis, with laparoscopy reserved for selected cases (10). In the study conducted in Zimbabwe, no cameras and monitors were used to document the magnified internal findings (3). This may have led to some diseases being overlooked. Given the availability of modern laparoscopy equipment, especially cameras and monitors for displaying magnified images, the causes of CPP were investigated, as well as the perioperative complications associated with diagnostic laparoscopy in a cohort in Zimbabwe.
Material and Methods
This cross-sectional study was conducted at the Parirenyatwa Group of Hospitals and Sally Mugabe Hospital in Harare, Zimbabwe, from January 1 to October 31, 2014. In total, 108 women with CPP were enrolled, 49 in the retrospective arm and 59 in the prospective arm. Participants were at least 18 years old and provided informed consent. Pregnant women and those who did not provide consent were excluded.
Retrospective arm: Hospital records of the patients who underwent diagnostic laparoscopy from January 1, 2014, to October 31, 2014, were retrieved. Sociodemographic characteristics, as well as gynaecological, obstetric, surgical, medical data, psychological history, laparoscopic findings, and perioperative complications were extracted onto an Excel spreadsheet.
Prospective arm: Participants who underwent ultrasonographic evaluation and diagnostic laparoscopy for CPP were recruited from the gynaecology outpatient clinic or wards. Laparoscopy was performed under general anaesthesia. Gas was insufflated using a Veress needle to 20–25 mmHg, which was used transiently only during Veress needle insufflation and primary port insertion, after which surgery was performed at pressures of 14-15 mmHg. Two additional 5-mm ports were placed in the right and left iliac fossae for pelvic and abdominal exploration. After the procedure, the pneumoperitoneum was released, and ports were removed under direct vision. The 10- and 5-mm ports were closed in two layers, with one layer closed using absorbable sutures. Intraoperative findings and complications were documented in an Excel spreadsheet. Participants were discharged and followed up within 2 weeks for any postoperative complications.
Case diagnosis: Pelvic inflammatory disease (PID) was diagnosed by the presence of tubal wall oedema, hyperaemia, exudation, or a pelvic mass, such as a tubo-ovarian abscess or perihepatic adhesions. Endometriosis was identified based on findings of classic blue-black “powder burn” lesions, non- classic clear or red “flame-like” lesions, peritoneal defects with endometriotic lesions, endometriomas, deeply infiltrating lesions, or histological confirmation. Ovarian cysts, uterine fibroids and pelvic congestion syndrome were confirmed by direct visualisation. CPP severity was assessed using an 11-point numeric rating scale of 0–10 (11). Participants were screened for depression or anxiety symptoms based on recommendations in the National Institute for Health and Clinical Excellence (NICE) guidelines (12).
Statistical analysis: Data were entered manually in an Excel spreadsheet before extracted onto Stata version 12.0 (Stata Corporation, College Station, TX, USA) for statistical analyses.
Ethical issues: Permission and ethical approval to conduct the study were granted by the Joint Research and Ethical Committee of the University of Zimbabwe Faculty of Medicine and Health Sciences and the Medical Research Council of Zimbabwe. Written informed consent was obtained from every participant.
Results
Summary of sociodemographic and clinical data: The mean age of the study participants was 33.3 years (range, 16–67 years), with a median parity of 2 (range, 0–7). Most of the participants were housewives (69.4%) residing in urban areas (86.1%). Almost half (48.2%) were educated up to secondary and tertiary levels.
Nature of CPP and associated symptoms: Participants described their pain as either moderate or severe. Most experienced intermittent pain (90.7%), while more than half had subfertility (54.3%).
Summary of symptoms associated with CPP: Dyspareunia was associated with pain in 15.7% of the women. Depression and anxiety were reported in 54.6%, and 84.7% reported increased family expenditure due to medical care costs.
Past medical history: In the preceding month, almost one-seventh of the participants visited a healthcare provider more than three times (69.5%), while over two-thirds received analgesia (67.8%) or antibiotics (64.4%). A minority of women (10%) had a prior history of abdominal or pelvic surgery.
Summary of preoperative ultrasound findings: More than one-third of the women (34.3%) had normal preoperative sonography, while almost half (40.7%) had ovarian cysts.
Summary of diagnostic laparoscopic findings: Ovarian pathologies were the most common findings at laparoscopy, mainly ovarian cysts (18.5%), adhesions (15.7%), and endometriosis (15.7%). The frequency of chronic PID was low (9.3%). Combined pathologies were noted in 15.7% of the participants, mainly fibroids, adhesions, PID, and endometriosis.
Summary of complications from diagnostic laparoscopy: The overall complication rate of diagnostic laparoscopy was 6/108 (0.06%), with complications including intraoperative uterine perforation (2/108; 0.02%) and postoperative port site sepsis (4/108; 0.04%).
Discussion
CPP is prevalent in reproductive-aged women and contributes to a significant proportion (20%) of gynaecological consultations in most health centres worldwide (13). In Egypt, 26.6% of gynaecological consultations were for CPP (14). However, data on the prevalence of CPP in Zimbabwe are lacking. A study conducted in Zimbabwe in 1991 found that 35% of women had reproductive pathologies on diagnostic laparoscopy (3). In this study, various pathologies were identified in 82% of women on diagnostic laparoscopy. We attribute this significantly higher rate to better laparoscopy equipment. Ovarian cysts were the most common finding on preoperative USS (40.7%), but only 18.5% were detected on diagnostic laparoscopy (18.5%). Most of the ovarian cysts detected on preoperative USS were possibly functional ovarian cysts Thus, repeat imaging before laparoscopy is vital. Most ovarian cysts identified on ultrasound were likely functional cysts, which explains the discrepancy between ultrasound and laparoscopic findings. It is also emphasised that ovarian cysts are often incidental and not necessarily causal in chronic pelvic pain. USS is the gold standard in the diagnosis of endometriosis (15). In this study, endometriosis was not diagnosed preoperatively, raising the issue of the quality of preoperative USS. Diagnostic laparoscopy identified endometriosis in 15.7% of women, similar to a study in India (16). However, this is low compared to current evidence showing that prevalence ranges from 15.4% to 71.4%, based on a comprehensive review of 69 studies (17). The evidence is variable due to heterogeneity in study design and selection bias. Our low prevalence may be due to limited camera resolution available at the time, absence of routine histological confirmation, under- recognition of subtle and deep infiltrating endometriosis, or operator-dependent diagnostic variability. Uterine fibroids were found in 6.5% and 3.4% of cases on USS and diagnostic laparoscopy, respectively. This percentage is lower than that reported in similar African studies (>60%) (18). This is possible because many fibroids in African women are intramural or submucosal and are not visible on USS (19). Small fibroids may not be detected with older ultrasound machines, and they are frequently incidental findings rather than the cause of CPP. This finding demonstrates that USS is a sensitive modality in the initial evaluation of uterine fibroids in CPP. Similar studies have shown that diagnostic laparoscopy identified uterine fibroids in 6.1%–8% of cases (16,20). Even though pelvic pain is a symptom commonly associated with uterine fibroids, most women with fibroids are asymptomatic; thus, a full evaluation for CPP is crucial to identify the aetiology of the pain, even with detectable fibroids. PID was diagnosed in one participant (0.9%) on USS, but was detected in 9.3% of CPP cases on diagnostic laparoscopy. This highlights the limitation of USS in the diagnosis of PID. The prevalence of PID was similar to that of another study conducted in a different setting. However, a study conducted in India identified PID in 40% and 47% of cases on USS and diagnostic laparoscopy, respectively (16). Proper diagnosis and management of PID is crucial as it can cause significant sequela, such as infertility, pelvic adhesive disease, and CPP. Adhesions were found in 15.7% of patients on diagnostic laparoscopy, as in a study in India (21). However, another Indian study reported adhesions in 7% of cases (16). Intraperitoneal adhesions were the most common diagnosis in patients with CPP (22). The low incidence of previous abdominal surgery and PID among participants may justify these findings. Overall, diagnostic laparoscopy is an effective method for diagnosing adhesions in women with CPP. Pelvic congestion was diagnosed in only 2 participants (1.9%) during laparoscopy, with no cases identified on preoperative USS. Similarly, a study reported pelvic congestion in 5% and 10% of cases on USS and laparoscopy, respectively (16). This discrepancy may be attributed to ethnic differences or USS quality. Conventional methods often miss varices, making selective ovarian venography the preferred approach, while non-invasive techniques like magnetic resonance imaging and duplex ultrasound are gaining popularity (23).
Most participants reported moderate to severe pain, consistent with findings in other studies (14,24). Depression and anxiety are common among women with CPP and are linked to factors such as severe pain and subfertility (25). Anxiety was twice as prevalent as depression in this group. Most women reported a poor quality of life due to CPP, influenced by mental health issues, multiple hospital visits, and financial strain. CPP negatively impacts women’s quality of life, with over 80% reporting financial burdens related to treatment (26,27). In our study, perioperative complications included intraoperative uterine perforation (2/108, 0.02%) and postoperative port site sepsis (4/108, 0.04%). A large study reported intraoperative and postoperative complications in 5.6% and 6.5% of women, respectively (28). Intestinal injuries were the most common (0.5%), indicating that laparoscopy is a reasonable method for managing CPP when performed by skilled practitioners.
Limitations
A key limitation of this study is that it was originally conducted as part of postgraduate academic research in 2014, with an initial focus on institutional audit rather than immediate publication. settings, including limited funding, lack of structural mentorship and heavy clinical workloads. Although the dataset was later revisited and refined, these factors may have affected the timelines of reporting and broader contextual relevance of the findings. At the time of this current study (2014), diagnostic laparoscopy was widely regarded as the reference standard, particularly in low-resource setting with limited access to advanced imaging. Current practice recommends expert transvaginal ultrasound as a first-line for suspected endometriosis, with laparoscopy reserved for selected cases. This study was partly retrospective and faced various challenges, such as data issues, recall bias and difficulty controlling confounding factors. Various practitioners conducted USS and laparoscopy, affecting the standardisation and quality of procedures. Furthermore, the study did not collect histological nor microbiological specimens and relied solely on subjective findings for diagnosing endometriosis and PID.
Strengths
Despite the delayed submission of the research work, the findings remain highly relevant, providing valuable baseline data on diagnostic pathways, disease patterns, and surgical safety of laparoscopy for chronic pelvic pain in a sub-Saharan African context. The study combined retrospective and prospective arms to obtain a comprehensive analysis of CPP and its underlying conditions, with well-defined diagnostic criteria, thereby enhancing the reliability of findings. The use of an 11-point numeric rating scale to assess pain severity in standardised evaluations. Furthermore, a follow-up period was implemented to assess postoperative complications and to analyse surgical outcomes. Finally, modern laparoscopy equipment was used in the evaluations.
Recommendations
Standardised diagnostic procedures are needed for the accurate identification of endometriosis and PID. Increasing access to diagnostic procedures such as laparoscopy for women in underserved areas is essential. Further studies into CPP and increasing awareness among healthcare providers and the public in low-income settings are also recommended.
Conclusion
This study found that CPP is frequently caused by ovarian pathology, endometriosis, and pelvic adhesions. Most women (81.6%) had a physical cause identified during diagnostic laparoscopy, highlighting its utility in the evaluation of CPP. The perioperative complication rate for diagnostic laparoscopy was low.
Acknowledgements
The authors would like to acknowledge the clinical staff members and theatre team who tirelessly invested time during the period of this study, as well as all the participants who willingly volunteered to be part of this study.
References
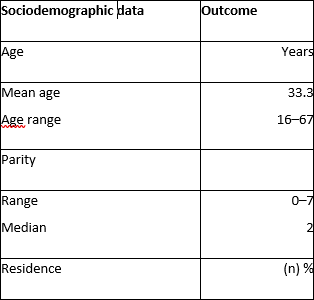
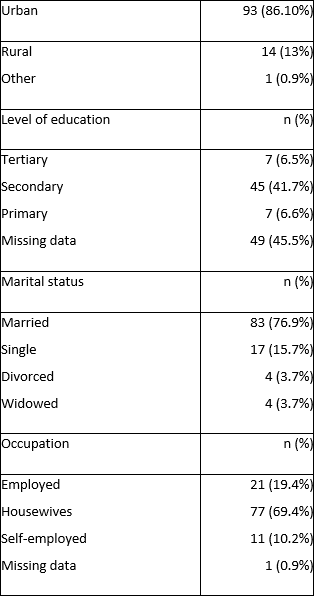
Table 1
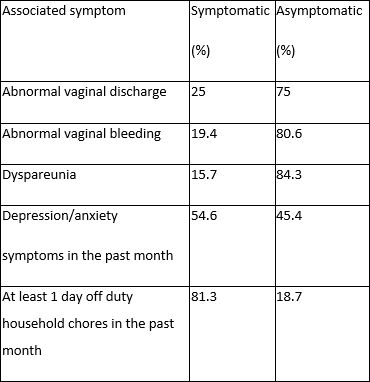
Table 2: Symptoms associated with CPP
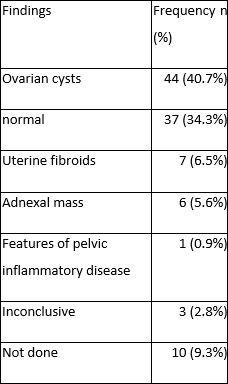
Table 3: Preoperative ultrasound findings