Authors / metadata
DOI10.36205/trocar7.2026006
Abstract
Pregnancy in the cornual region has been considered a type of ectopic pregnancy, accounting for 2%–5% of such cases. This location, currently recognized as eutopic, is considered by some reports to be a risk factor associated with serious complications: uterine rupture and difficult-to-control hemorrhage. Currently, pregnancies in the cornual region are subclassified into three types: (a) cornual, (b) interstitial, and (c) angular. Early diagnosis is key to the conservative management of this type of pregnancy, as a late diagnosis increases the possibility of rupture and hemorrhage, which would result in a high probability of requiring a hysterectomy. Conservative treatment is performed through careful case selection, with the use of methotrexate, mifepristone and other drugs. Minimally invasive surgery has also been used, either initially or as a complementary procedure. This article details a very specific case of a pregnancy in the cornual region treated with methotrexate. Because the ß-hCG levels never became negative at five-month follow-up, and the ultrasound exams continued to report the presence of a gestational sac in the cornual region, it was decided to perform an operative hysteroscopy.
Study Objective: To present the clinical case of a rare pathology, in which resolution was achieved using a minimally invasive approach.
Design: Case report.
Introduction
Ectopic pregnancy (EP) is defined as the implantation of a blastocyst that develops outside the endometrial cavity. Pregnancies in the cornual and interstitial regions represent 2% to 5% of EP. By definition, EP refers to implantation and development of a gestational sac in the proximal and lateral regions of the uterus, also known as uterine horns. These carry a high risk of rupture, hemorrhage, and even death (1). All EP occurring in the cornual region of the uterus have been considered as “cornual” ectopic pregnancies. It is important to note that three terms are currently used to describe this type of pregnancy: (a) cornual, (b) interstitial, and (c) angular. The findings in imaging studies, management, and results may be different (1,2). According to the medical literature, imaging specialists and gynecologists often do not distinguish between interstitial and cornual pregnancy, using both terms interchangeably (2). Currently, it is recommended to classify as a cornual ectopic pregnancy, a pregnancy that implants in a rudimentary “horn” of a uterus with some type of Müllerian malformation (unicorn uterus, bicornuate uterus, septate uterus) (3). Ultrasound criteria for diagnosing an ectopic pregnancy in the cornual region include: an empty endometrial cavity, an eccentrically located gestational sac (approximately 1 cm from the lateral uterine wall), and a thin layer (<5 mm) of myometrium surrounding the sac. This type of pregnancy carries a significant risk of rupture due to the lack of myometrial support surrounding the gestational sac (1,2,3). An interstitial EP is the one in which the blastocyst implants in the interstitial portion of the fallopian tube and near the uterine myometrium, located laterally to the round ligament, and surrounded by less than 5 mm of myometrium, and presents an ultrasound sign of an interstitial line that appears in the first trimester of pregnancy. The interstitial region is susceptible to rupture due to an increase in distension and hypervascularity. For this reason, it is imperative that the EP is diagnosed early, in the first trimester of pregnancy, for conservative treatments (1,2,3). An angular pregnancy is a third type of pregnancy implanted in the cornual region of an anatomically “normal” uterus. It is implanted medial to the round ligament, in the lateral angle of the endometrial cavity and medial to the uterotubal junction. This type of pregnancy can reach term. The thickness of the myometrial layer is > 5 mm, and there is no sign of an interstitial line. Approximately 29% of angular pregnancies in the cornual region end in a uterine rupture, although a recent prospective study that included 42 cases, the authors found that 80% of these pregnancies reached term and 20% ended in early abortions. In addition, they reported no complications of uterine rupture, maternal death, abnormal placentation, or need for hysterectomy (3,4,5). Another reason why an angular pregnancy is considered a type of EP in other publications is the difficulty in differentiating an interstitial pregnancy from an angular pregnancy, especially during the first trimester. It also presents symptoms similar to a typical ectopic pregnancy (4). The angular pregnancy is a poorly recognized entity, with approximately 100 cases reported in the literature. Complications are reported, with an estimated 28.5% of cases ending in uterine rupture, and 20% in spontaneous abortion. Although the angular pregnancy could be considered a potentially viable intrauterine pregnancy, the risk of uterine rupture is not negligible and could lead to massive hemorrhage, with a maternal mortality rate of 5% (3,4). However, one of the best practice recommendations of the European Society of Human Reproduction and Embryology (ESHRE) published in 2020 recommends that the term “angular pregnancy” should be abandoned (6). In all three types of pregnancy in the cornual region, early diagnosis in the first trimester is key to more appropriate management and to avoid complications related to rupture and hemorrhage, which could even lead to mortality. The diagnosis, as with other types of EP, is based on studies and imaging -ultrasound, clinical suspicion, and human chorionic gonadotropin hormone levels (3,4). The use of 2-D and 3-D transvaginal ultrasound and the experience of the imaging specialist are crucial for the correct diagnosis of the three types of pregnancies located in the cornual region. When there is insufficient experience or the result is ambiguous, the use of other diagnostic methods such as magnetic resonance imaging is recommended (3,4). Currently, conservative medical and surgical approaches are used to achieve the best outcomes for the three types of EPs in the cornual region of the uterus. Of the conservative approaches, pharmacological treatment based on local or systemic methotrexate has been effective in the majority of reported cases in patients who meet criteria for its application. Tanaka et al. were the first to describe the use of methotrexate for the medical and pharmacological treatment of ectopic pregnancy in the cornual region (7). Hysteroscopic resection of cornual pregnancy is a minimally invasive technique, an alternative approach that allows for the visualization and removal of all pregnancy products without affecting the rest of the uterus. The first report of hysteroscopic resolution of cornual ectopic pregnancy is attributed to Meyer et al., who described the hysteroscopic technique using a laparoscopic approach (7,8).
Case report
A 33-year-old patient with a diagnosis of uncomplicated EP in the left cornual region (7 weeks by last menstrual period) was treated medically with a single systemic dose of methotrexate (X mg/kg body weight), showing a good initial response.
Measurements and main results
However, during the five-month follow-up, β-hCG never became negative and transvaginal ultrasound reports continued to report the presence of a gestational sac in the left cornual region. Notably, one month after methotrexate administration, the patient resumed regular menstrual bleeding of normal volume (Table 1: Record of the evolution of the β-hCG in the follow-up carried out at five months).
It was decided to perform a diagnostic-surgical hysteroscopy, for which a Bettocchi-type hysteroscope (Karl Storz SE & Co KG,Tuttlingen, Germany) was used, with saline solution as a distention medium. An occlusion of the left cornual region was observed, with a fibrous adhesion lateral to the left ostium. A structure corresponding to a degenerated gestational sac was seen. A cold section of the aforementioned adhesion was performed, and the gestational sac was subsequently removed with 5 Fr grasper forceps, which emerged intact.
It was speculated that the fibrous uterine synechiae might resemble a rudimentary uterine horn in an anatomical configuration and therefore be clinically and sonographically indicative of a cornual pregnancy. One week after hysteroscopy, a new β-hCG quantification was performed, showing a value of 2 mIU/ml (negative). Traditionally, treatment of an EP in the cornual region involved hysterectomy or cornual excision via laparoscopy or laparotomy. Currently, it is considered that, depending on the individualization of each particular case, a conservative treatment can be offered based on the systemic application of methotrexate, with a success rate of between 89% and 98%. It has been reported that at least one in seven patients with cornual ectopic pregnancy treated with methotrexate may require additional surgery. Hysteroscopic resection of pregnancy in the cornual region is an alternative minimally invasive approach that allows direct visualization and removal of all products of gestation, without affecting the rest of the uterus. The first hysteroscopic resection of this type was reported by Meyer et al. (1989), performed after laparoscopic confirmation. Sanz et al. (2002) further expanded the concept using hysteroscopy under ultrasound guidance and Pal et al. performed a hysteroscopic resection of the gestational sac and subsequently removed the excised products of pregnancy by suction under combined ultrasound and laparoscopic guidance (8,9,10,11,12). More recent reports of successful hysteroscopic resection of pregnancy are indicative of the potential of this technique as an alternative with a reduced impact on future fertility and maternal outcomes (9,10). In selected cases, hysteroscopic excision may serve as an alternative or complementary treatment for cornual ectopic pregnancy. To our knowledge, and based on a review of the medical literature, this is the first reported case of hysteroscopic resolution performed without the use of energy (resector), using only a 5 Fr grasper. Likewise, laparoscopic or ultrasound guidance were not necessary. The histopathological report of the operative specimen was reported as fibrosed first trimester villi, hyalinized gestational sac. In the ultrasound follow-up after hysteroscopy, a gynecological ultrasound reported no evidence of endometrial alterations of 10 mm. Ten months after the intervention, the patient achieved a new spontaneous pregnancy with eutopic intrauterine implantation. The gestation is uneventful.
Conclusion
In this case, an EP in the cornual region was associated with a fibrous synechia, adhesion, that almost completely occluded the left side. Despite an initially good response to the application of methotrexate, ß-hCG never became negative in the five-month follow-up, and ultrasound studies continued to report the presence of a gestational sac in the cornual region. Hysteroscopy is a minimally invasive alternative for selected cases of ectopic pregnancy in the cornual region and serves as a useful complementary tool to conservative treatment with methotrexate.
References
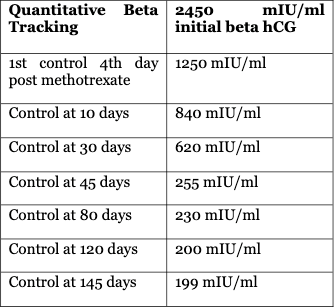
Table 1: Evolution of β-hCG/five monts
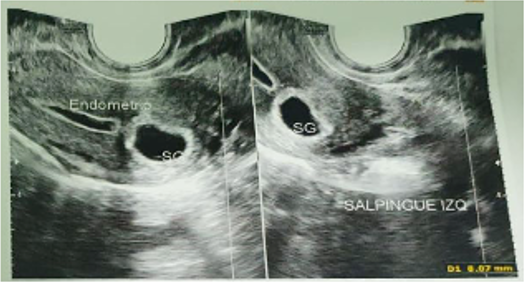
Figure1: Transvaginal ultrasound at 5 months after treatment with methotrexate continued to report the presence of a gestational sac in the cornual region
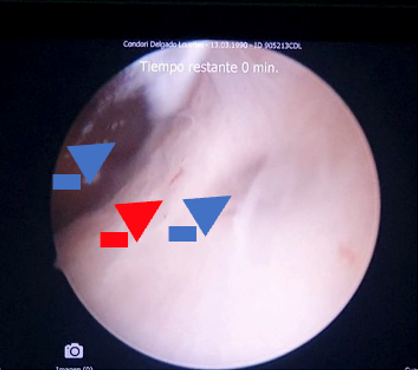
Figure 2: Left cornual region occluded by fibrous uterine synechiae, the blue arrow indicates entry into the cornual region. The red arrow indicates fibrous synechiae that almost completely occluded the left cornual region. The blue arrow indicates the uterine cavity
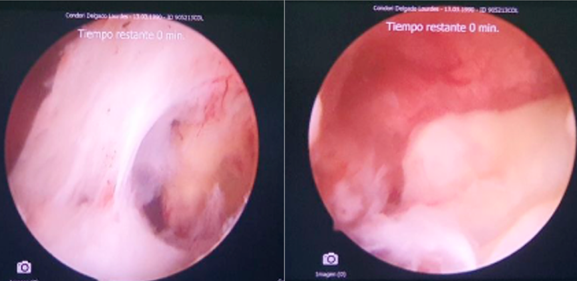
Figure 3: After blunt entry maneuvers, it is possible to visualize the structure corresponding to a degenerated gestational sac that is located lateral and close to the left osteum. After the cold section of the synechia, it is possible to reach the gestational sac
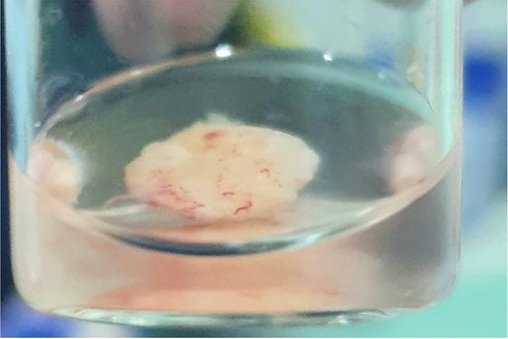
Figure 4: Complete extraction of the gestational sac is achieved through blunt maneuvers, grasping and retraction under hysteroscopic visualization of the gestational sac